Tongue tie (ankyloglossia) occurs when the band of tissue connecting the underside of the tongue to the floor of the mouth is too short, too tight, or attached too far forward—restricting the tongue's normal movement. This common condition affects 4-10% of newborns and can cause significant feeding difficulties in infants, speech delays in children, and lifelong challenges with oral function. At Dental Sedation Ottawa, we perform precise, gentle tongue tie release procedures that immediately restore tongue mobility—with comprehensive sedation options ensuring complete comfort for patients from newborns to adolescents.
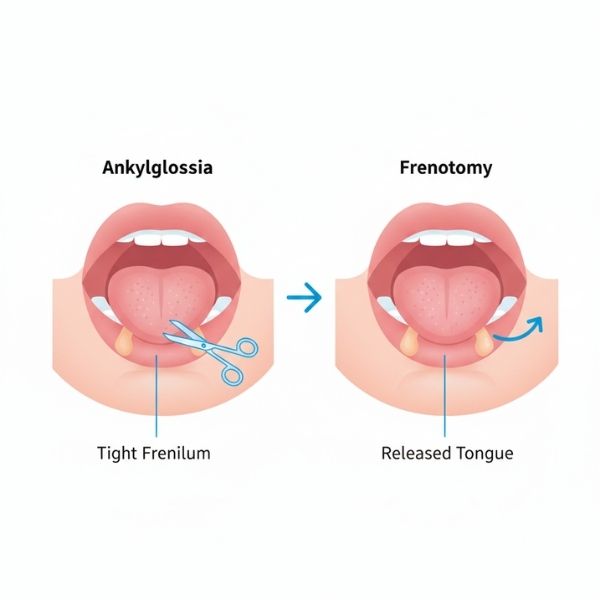
Tongue tie, medically called ankyloglossia, is a condition present from birth where the lingual frenum (the thin membrane under the tongue) restricts tongue movement. In normal anatomy, this frenum should be thin, flexible, and attached well back from the tongue tip. With tongue tie, it's either too thick, too tight, too short, or attached too close to the tip of the tongue—or a combination of these factors.
Think of the tongue as needing to move like a windshield wiper—sweeping side to side, reaching up to the roof of the mouth, and extending forward past the lower teeth. When the frenum tethers it down, the tongue can't perform these essential movements properly. This restriction affects feeding (especially breastfeeding), speech development, oral hygiene, eating, and even social development.
Tongue ties range from mild (slight restriction) to severe (tongue completely anchored to the floor of the mouth). Some are immediately obvious—you can see the tight band of tissue. Others are "posterior tongue ties" located further back under the tongue and harder to spot visually but equally problematic functionally.
The condition runs in families (genetic component) and affects boys more often than girls (about 2-3:1 ratio). It occurs across all ethnicities and socioeconomic groups.
Ready to learn more? Schedule a consultation today.
At Dental Sedation Ottawa, we understand that the idea of oral surgery on your baby or child can feel frightening. However, tongue tie release is one of the quickest, simplest procedures we perform—and with appropriate anesthesia and sedation, it's completely painless and often takes just minutes.
For babies under 4 months old, we often use only topical numbing gel. The procedure is so quick (literally 1-2 minutes) that many newborns sleep through it or cry only briefly during the release itself. Parents can immediately comfort, hold, and nurse their baby afterward. This is the most common approach for infant tongue tie related to feeding difficulties.
For older infants (6+ months) and toddlers, we combine local anesthetic injection (to ensure complete numbness) with nitrous oxide (laughing gas) to help the child stay calm and still. The child remains awake but relaxed.
Learn more about nitrous oxide →Medication taken before the appointment creates drowsiness and reduces anxiety significantly. Good for anxious toddlers and young children. Your child remains responsive but deeply relaxed and often won't remember the procedure.
Explore oral sedation →Deeper sedation for high anxiety, children who cannot cooperate, or when the tongue tie is complex and requires more extensive release. Administered through a tiny IV line with continuous monitoring.
Discover IV sedation →Complete, peaceful sleep with zero awareness. Administered by board-certified medical anesthesiologists (Dr. Hesham Talab, MD MSc PhD FRCPC FASE and Dr. Asad Mirghassemi, MD MSc FRCPC). Best for severe dental anxiety, special needs children, very uncooperative toddlers, or when extensive dental work is needed along with tongue tie release. Hospital-grade safety in our clinic.
Learn about general anesthesia →If your child needs other dental procedures—fillings, crowns, extractions, cleanings—we can perform tongue tie release during the same sedated appointment. One visit, one recovery period, significantly less overall stress.
Questions about your options? We're here to help.
Tongue tie's most immediate and serious impact occurs with breastfeeding. The tongue must cup and wave in a specific motion to compress the breast and transfer milk effectively. Restricted tongue movement disrupts this process, causing:
As children grow, tongue tie that wasn't addressed in infancy can significantly impact speech development:
Ready to take the next step? Our team is here for you.
Frenum attaches at or very near the tongue tip. Usually thin and highly visible. Often called "classic tongue tie." Very restrictive and easily identified.
Frenum attaches 2-4mm behind tongue tip. May be thin or thick. Moderately restrictive.
Frenum attaches in the middle or back third of the tongue underside. Often thick, broad, or shiny rather than a thin band. Can be harder to see visually but very functionally restrictive. Sometimes missed by providers unfamiliar with posterior ties.
Frenum is completely buried under mucous membrane. Not visible at all but severely restrictive. Requires experienced provider to identify through functional assessment rather than visual inspection.
Important: Severity of restriction doesn't always correlate with visual appearance. Some posterior ties that look minor are functionally devastating. Functional assessment (how does the tongue actually move?) matters more than appearance.
Before the procedure, we perform a comprehensive evaluation including visual examination of the frenum's thickness, attachment point, and appearance, functional assessment of tongue's range of motion, review of feeding difficulties, speech problems, or other symptoms, and for infants, often a feeding observation to see how tongue tie affects nursing.
On the day of the release, we begin by administering appropriate anesthesia/sedation based on your child's age and needs. For young infants, topical gel often suffices. The practitioner gently lifts the tongue to expose the frenum fully. Using surgical scissors or a scalpel, we make a quick cut through the frenum, releasing the restriction. For simple, thin frenums, this takes literally seconds (10-30 seconds). Some blood appears but usually stops within 1-2 minutes.
For thicker or more complex frenums, the release may require cutting through multiple tissue layers and occasionally placing 1-2 dissolvable stitches. Even complex releases typically take only 5-10 minutes. Some practitioners use laser technology (CO2 or diode lasers) for tongue tie release, which can cauterize blood vessels simultaneously, reducing bleeding.
We apply gentle pressure to stop any bleeding, demonstrate the tongue's new range of motion, teach stretching exercises essential for preventing reattachment, and for infants, encourage immediate nursing or bottle feeding for comfort and to begin using the newly mobile tongue.
Time Required: Simple infant tongue tie release: 1-5 minutes. Complex releases or procedures in older children: 10-20 minutes.
Ready to get started?
Breastfeeding or bottle feeding immediately after the procedure helps with comfort and begins the relearning process. Some babies latch better immediately; others need 3-7 days to learn to use their newly mobile tongue effectively.
Working with a lactation consultant within the first week after release optimizes outcomes.
The most important part of aftercare is stretching exercises to prevent the frenum from reattaching during healing. Without exercises, reattachment occurs in 5-20% of cases.
We teach you to gently lift your child's tongue to stretch the release site 4-6 times daily for 2-4 weeks. We demonstrate thoroughly and provide written instructions with photos.
Ready to take the next step? Our team is here for you.
Depending on complexity and sedation needs
Many insurance plans cover tongue tie release at 50-80% when medically necessary due to documented feeding difficulties, failure to gain weight, speech delays, or dental health concerns. Some provincial health plans provide coverage for infant frenectomy when feeding problems are documented by lactation consultants or pediatricians.
We provide direct billing to major insurance carriers and accept the Canadian Dental Care Plan (CDCP). Our team reviews your insurance coverage during consultation.
"Dr. Koniouchine, simply put, is fantastic. 10/10."
— Julie Lacelle
"I had an emergency case with my son and Dr. Alimova was so kind to squeeze us in between her patients and provide us with the best service. Even though like many kids in his age afraid of doctors she was able to find approach to him. I highly recommend her!"
— Zukhra Turakulova
"Staff was friendly, efficient and technically skilled. My extraction was as painless as it gets."
— Conor Middleton
"Great place, very good attention to details. Made us comfortable knowing that our son would have the best care."
— Lynn Thibault
Dentist Referrals Welcome: We collaborate with referring dentists, pediatricians, lactation consultants, and speech therapists throughout Ottawa and Eastern Ontario.
Learn About Our Referral Process